Pro-Agility 5-10-5 Shuttle
The Pro-Agility Test (also known as the 5-10-5 shuttle or 20-yard shuttle) is a rapid back-and-forth shuttle run that measures linear acceleration, deceleration, and lateral change-of-direction ability⁶.
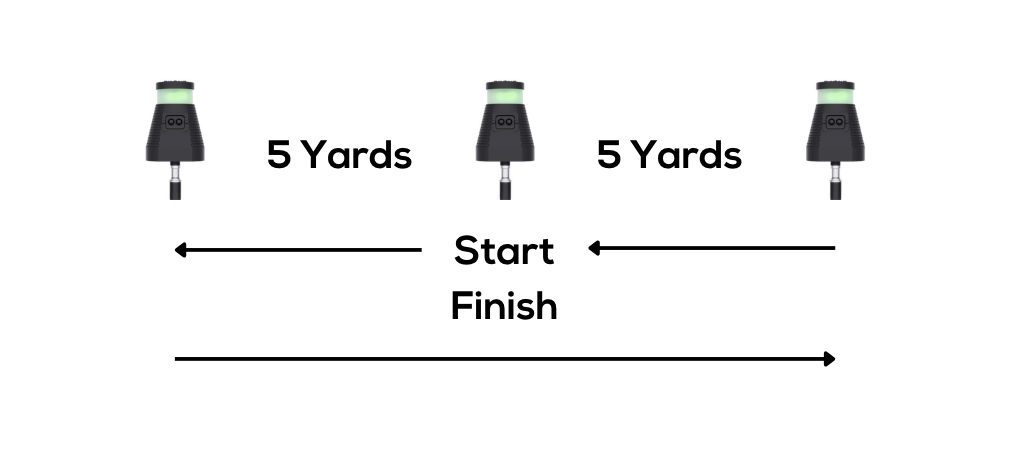
Setup: Place three timing gates in a straight line, 5 (4.5 metres) yards apart. The middle gate is at the start/finish line. Alternatively, the set up can involve one timing gate at the start/finish line and cones 5 yards apart on either side. Multiple gates allow for split times to give more data.
Start Position: The athlete straddles the start line in a 3-point stance. The down hand must correspond to the initial direction of travel⁶.
Procedure: On the cue, the athlete sprints 5 yards to one side, touches the line at the far cone with their hand, then changes direction, sprints 10 yards to the far cone on the opposite side, touches that line, and finally turns back and sprints 5 yards to finish⁶.
Trials: Perform in each direction; record best time for each. Compare left-versus-right times to detect asymmetry.
Scoring and Norms: Elite athletes often complete it in just over 4 seconds. Recreational athletes around 5 seconds are good, slower times suggest deficits. Discrepancies >0.2–0.3 s between directions may indicate a meaningful asymmetry.
T-Test Agility Drill
The Agility T-Test is widely used to assess multi-directional agility including forward sprinting, lateral shuffling, and backward running⁶.
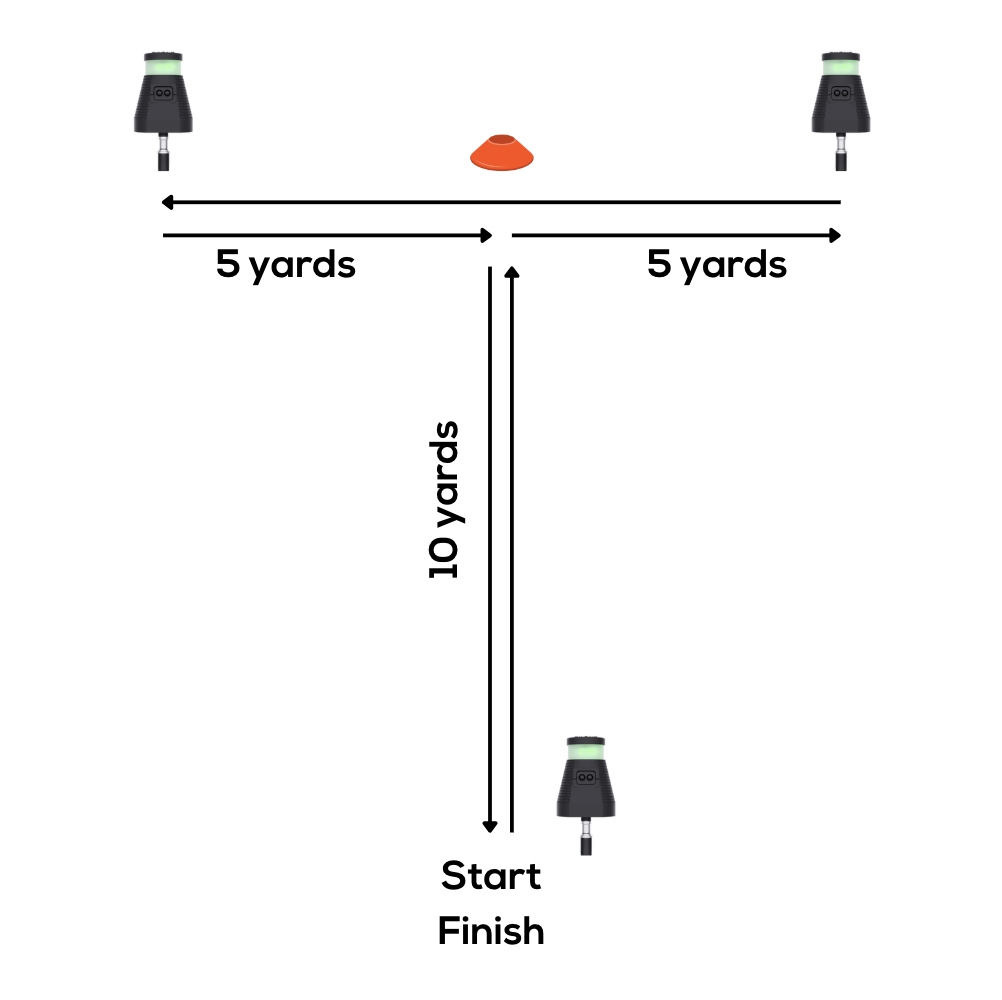
Setup: Gates in a T-formation: Start position A, position B (10 yards ahead), C and D (5 yards left/right of B). Timing gates at A, C and D. Alternatively, the set up can involve one timing gate at the start/finish line and cones at the other points. Multiple gates allow for split times to give more data.
Procedure: Sprint A→B, shuffle left to C, shuffle right to D, shuffle back to B, backpedal to A⁶.
Scoring: For adult athletes, ~10 seconds or less is common for high performers. Kyritsis et al.⁵ used a cutoff of 11 seconds in pro soccer.